
Point-of-Care Ultrasound for Soft Tissue
Michael Schick DO, MA
Point-of-care ultrasound (POCUS) is a diagnostic or therapeutic ultrasound done at the bedside, by a clinician, to answer a specific clinical question. POCUS for soft tissue complaints is well established in the emergency department and incredibly applicable in the primary care setting. Skin and soft tissue infections (SSTIs) are particularly common in a population with high rates of comorbid illnesses such as diabetes, venous stasis, lymphedema, and a growing prevalence of antibiotic resistance such as MRSA. A study of ED visits from 1996 to 2005 found that visits for abscesses more than doubled during that time, from 1.2 million in 1996 to 3.28 million in 2005(1). A similar study of both EDs and ambulatory care settings found that visits for abscess or cellulitis increased from 17.3 to 32.5 visits per 1000 patients from 1997 to 2005(2). Categorizing the complaint as infection or not, abscess or cellulitis, identification of a foreign body, and visualizing the extent of the illness is crucial in management. Decisions for antibiotics, incision and drainage, and referral are easily made with POCUS.
POCUS is an ideal modality to categorize SSTIs. A 2006 prospective study of 126 ED patients with soft-tissue infections assessed physicians’ clinical assessment and management plan before and after POCUS was performed. The authors found that 56% of patients had a change in management by detection of occult abscesses, prevention of invasive procedures, or guidance of further imaging or consultation(3).
Technique
- Clean all equipment well with germicidal wipes.
- Turn the machine on and select the high frequency probe/transducer. Choose the soft tissue or alternatively the vascular exam or small parts setting.
- Apply ample gel to the area of interest.
- Apply a sterile Tegaderm to the probe.
- Begin scanning in an area that appears normal on physical exam. This way you have an excellent comparison of normal and abnormal tissue.
- Image slowly with applying minimal pressure to reduce discomfort to the patient. Scan the area in its entirety in both the longitudinal and transverse planes.
- Use adequate depth. Explore shallow and deep fields so important pathology is not missed.
- Follow the findings. If an abscess is identified, continue to scan to better categorize its extent, size, depth and possible involvement of surrounding structures.
- Identify surrounding anatomy. Abscesses or foreign bodies can encompass or overly vessels, tendons, bones, etc. Use Color Doppler before doing a procedure to identify vessels and avoid iatrogenic injury.
- Utilize appropriate gain. Gain changes how bright the gray scale image is. A decent rule to follow is vessels should look anechoic or black.
NORMAL ANATOMY
First, know what normal anatomy looks like on ultrasound. Knowing normal will make it simple to identify pathology. As identified in figure 1, the epidermis is hyperechoic and most superficial or closest to the probe. The next layer is hypodermis, which contains mostly subcutaneous fast and is generally hypoechoic compared to epidermis or fascia. The hypodermis is the typical location where cellulitis will occur. Below the hypodermis a layer of bright or hyperechoic fascia separates the next layer of muscle. Muscle will appear hypoechoic compared to fascia or epidermis and has a typical striated appearance. Just above, below, or with in the muscle layer vessels and nerves are typical identified. However, depending on where you are imaging in the body there may be both superficial and deep blood vessels above and below the muscle layer. Vessels appear anechoic or black on ultrasound. Below the muscle layer you may identify another facial layer followed by bone. Bone appears bright or hyperechoic and will typically shadow.
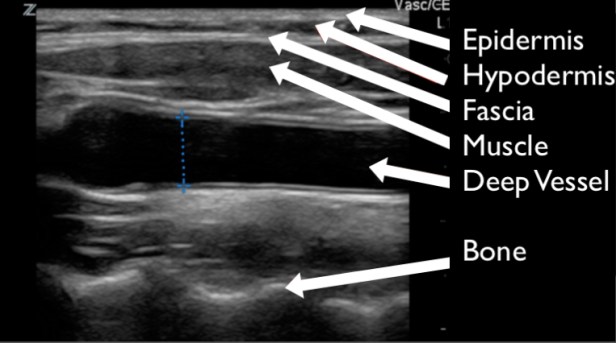
FIGURE 1. THE APPEARANCE OF NORMAL SOFT TISSUE ON A GRAY SCALE ULTRASOUND. THIS PARTICULAR IMAGE IS TAKEN IN A SAGITAL PLANE OF THE NECK.
CELLULITIS AND ABSCESS
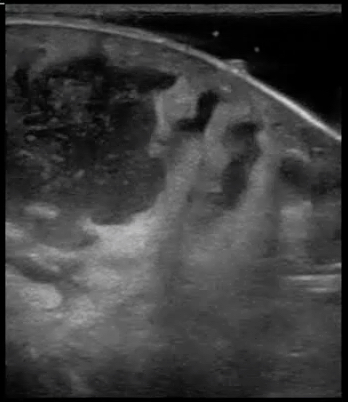
The most common finding related to SSTIs in POCUS is cellulitis. Cellulitis is a soft tissue infection primarily involving the hypodermis space. In cellulitis, the immune system responds to a bacterial infection in the superficial soft tissue. A cascade of white blood cell and inflammatory marker activation leads to the hypodermic space filling with serous fluid. On physical exam this typically appears as an edematous, warm, and erythematous region of the body. On POCUS, direct visualization of the hypodermis demonstrates edema within the hypodermis. Fluid can be seen surrounding areas of fat within this space, but unless there is an abscess the fluid will not collect in one particular location. As fluid snakes around fat within the hypodermic space it gives the appearance of a cobblestoned street on ultrasound. Figures 2 and 3 demonstrate “cobblestoning”. Compare this image to the thin, homogenous hypodermic layer in figure 1 and you will appreciate how easy it is to identify cellulitis. An important caveat is that patients who have hypodermic edema chronically for other reasons such as from congestive heart failure, end stage renal disease, nephrotic syndrome, liver disease, etc. will also take on a “cobblestoning” appearance in their dependent body regions. This highlights the importance of physical exam and how POCUS needs to be interpreted within the clinical context.
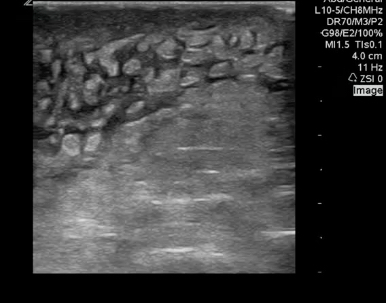
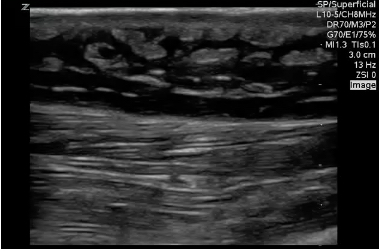
FIGURES 2 AND 3. TYPICAL APPEARANCE OF “COBBLESTONING” IN CELLULITIS. ANECHOIC OR HYPOECHOIC EDEMA IS SEEN WITHIN THE HYPODERMIS, SURROUNDING AREAS OF SUBCUTANEOUS FAT.
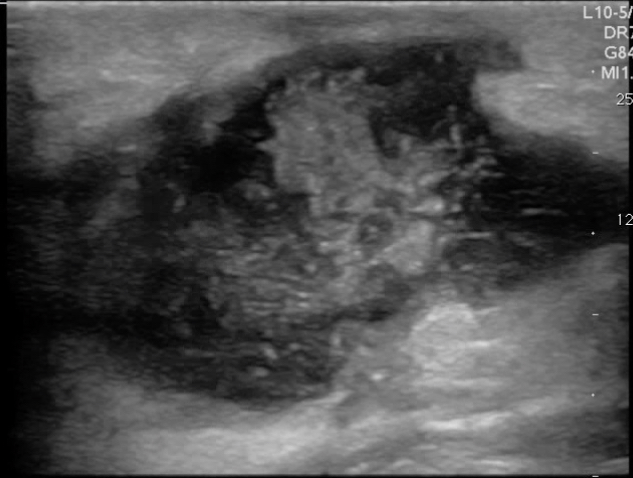
An abscess is a collection of pus or dead white blood cells in response to a SSTI. Antibiotics may be ineffective as a primary treatment and POCUS can help identify which patients require incision and drainage. In contrast to cellulitis, the typical appearance of an abscess on POCUS is an anechoic collection of fluid. There may be some internal echoes as dense pus or internal debris may coalesce. Occasionally, the debris or pus may be so profound that the abscess almost appears like soft tissue. When this occurs, adding downward pressure to the ultrasound transducer will make the pus move around. This is often called a “swirl sign” and helps identify the abscess. Importantly, POCUS allows the clinician to identify the coexistence of cellulitis and abscess or an isolated abscess and unnecessary antibiotics may be avoided. Figure 4 and 5 demonstrate the typical appearance of abscesses with POCUS.
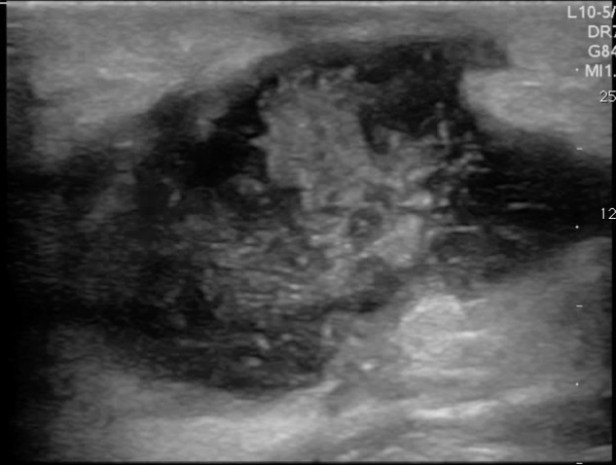
FIGURES 4 AND 5. TYPICAL APPEARENCE OF ABSCESSES WITH POCUS. ANECHOIC OR HYPOECHOIC COLLECTION OF FLUID WITH INTERNAL ECHOES FROM PUS/DEBRIS.

FIGURE 6. COBBLESTONES
Hands, feet, fingers, and toes can be difficult to image. It can be challenging to apply adequate gel to these irregular surfaces and pain can limit the examination, particularly in pediatric patients. Utilizing a water bath can greatly facilitate the exam and visualization of pathology. The transducers are water proof and water is the perfect acoustic window. To use a water bath, fill a clean container with warm water and place the area of interest inside. If the patient can rest the body part on the bottom of the container it helps avoid movement. Place the probe inside and reduce the depth on the ultrasound machine until the area of interest is within view. Touching the patient’s skin with the transducer within the water bath negates the reason for using it, so image the body area with some water between the probe and skin. Figure 7 demonstrate the use of water bath. Water will appear anechoic with occasional echoes that are usually air bubbles.
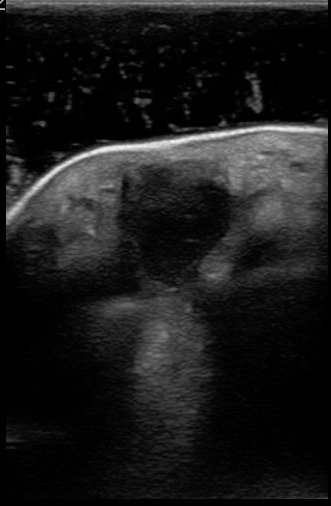
FIGURE 7. DEMONSTRATION OF A WATER BATH AND IDENTIFICATION OF A SOFT TISSUE ABSCESS IN THE HAND.
Now that you have identified an abscess the immediate reaction is to stick a knife in it right? Before that however, apply color flow to the abscess. If the abscess is adjacent to a vessel the entire area may appear anechoic and vessels can look like part of the abscess. Using color flow will identify the blood vessel and avoid iatrogenic injury.
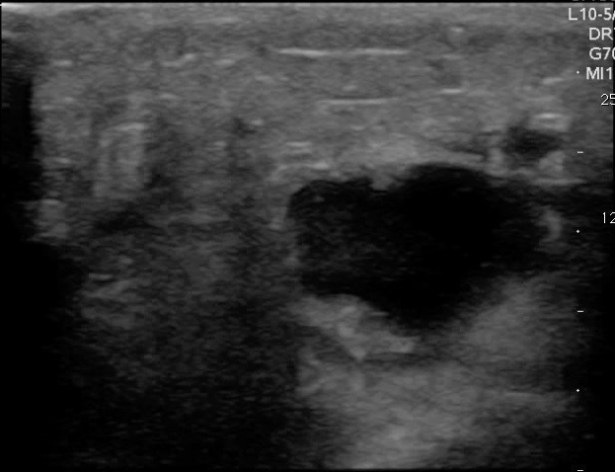
FIGURE 8. ABSCESS WITHOUT COLOR FLOW INTERROGATION.
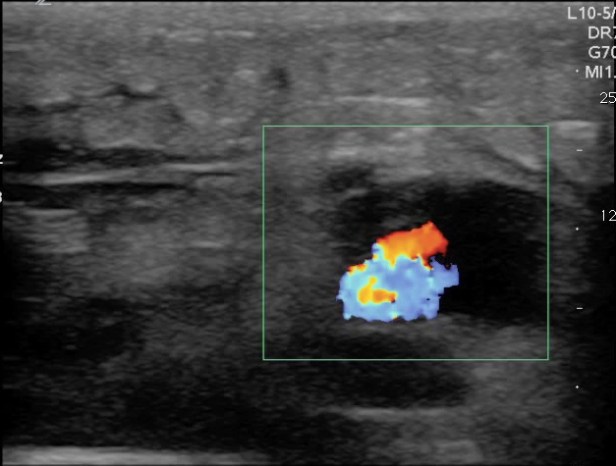
FIGURE 9. THE SAME ABSCESS WITH COLOR FLOW INTERROGAITON DEMONSTRATING AN ADJACENT BLOOD VESSEL.
Another reason not to immediately perform an incision and drainage is that the thing that looks like an abscess is actually something else! Many things can mimic an abscess such as masses, hernias, hematomas, pseudoaneurysms, and inflamed lymph nodes. POCUS can easily differentiate between these entities. Lymph nodes appear as small contained circular or oval shaped structures that have relatively hyperechoic centers and hypoechoic peripheries on ultrasound. They are typically referred to having the appearance of mini kidneys. Figure 10 demonstrates the classic appearance of a lymph node.

FIGURE 10. LYMPH NODE ON ULTRASOUND. MAY HAVE AN ANECHOIC CENTER SURROUNDED BY A HYPERECHOIC MIDDLE AND HYPOECHOIC PERIPHERAL LAYER.
What if you are imaging an abscess or cellulitis and you identify something bright or hyperechoic you do not recognize? Air is a poor conductor of ultrasound waves and appears very hyperechoic and creates a “dirty shadow” deep to the air. This is not a very sensitive test for necrotizing fasciitis, but is specific. Every patient who I have identified subcutaneous air in has gone emergently to the operating room. Figure 11 demonstrates the hyperechoic appearance of air. A large collection of air may create a classic reverberation artifact as demonstrated in figure 12.
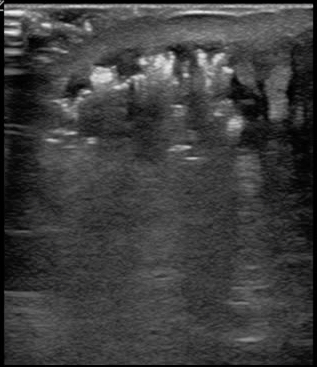
FIGURE 11. HYPERECHOIC AIR COLLECTING IN THE SUPERFICIAL PORTIONS OF A PATIENT’S SOFT TISSUE INFECTION. CONSISTENT WITH NECROTIZING FASCIITIS.
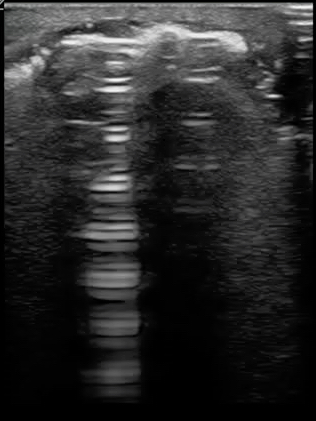
FIGURE 12. REVERBERATION ARTIFACT FROM A LARGE COLLECTION OF AIR IN A PATIENT’S SOFT TISSUE INFECTION. CONSISTENT WITH NECROTIZING FASCIITIS.
FOREIGN BODIES
Patient’s history for retained foreign bodies (FB) can be misleading. Many times patients may believe they have a retained FB, but it was just a puncture wound. Other times it may not be clear what type of FB is present and X-ray will miss any non radiopaque FBs. FBs can cause significant pain and can be a source of infection, especially organic FBs. Blind attempts at removal can lead to iatrogenic injury and have poor success rates unless large incisions are created for direct visualization. POCUS can identify organic and nonorganic FBs, identify adjacent anatomy, and guide extraction. FBs typically are hyperechoic on ultrasound and create a clean shadow. Ultrasound guided removal of FBs utilizes a similar technique to other ultrasound guided procedures:
- Pre-scan the patient with the high frequency transducer to identify the FB, its size and shape and surrounding structures (plan your extraction). Note the depth of the FB and keep that in mind while instrumenting the patient.
- Clean the patient and probe. Apply a probe cover.
- Use your non-dominant hand to hold the ultrasound transducer and visualize the FB. Using an in-plane approach, anesthetize the skin, the track that will be used to extract the FB, and then apply anesthetic above and below the FB. This will improve visualization, dissect the tissue around the FB to aid removal, and improve patient comfort.
- Most FBs are less than 2 cm in depth. If the FB is superficial removal with a blunt instrument such as a hemostat may be attempted now under direct ultrasound visualization.
- If the attempt is unsuccessful placing at least one needle in the patient with the tip against the FB can facilitate guidance. If the FB is large or oddly shaped a small incision may be required for removal.
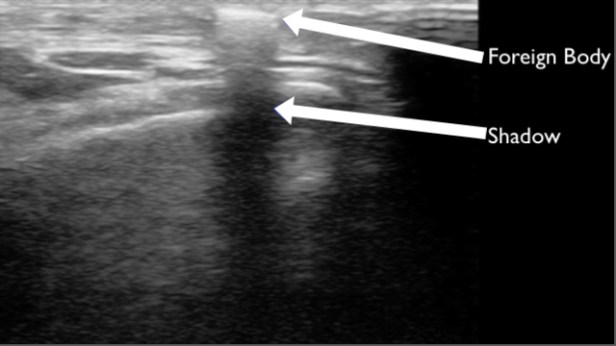
FIGURE 13. SUPERFICIAL FOREIGN BODY IDENTIFIED AS A HYPERECHOIC LINEAR STRUCTURE IN THE SUPERFICIAL TISSUE WITH SHADOWING. AFTER REMOVAL IT WAS IDENTIFIED AS A PIECE OF GLASS.

FIGURE 14. A LONG LINEAR FOREIGN BODY IDENTIFIED AS A SHISH KEBAB SKEWER AFTER EXTRACTION.
Notably, very small FBs may be missed with POCUS or may be obscured by subcutaneous air or hematoma. Deep FBs are particularly difficult to extract and multiple attempts can cause significant soft tissue injury. Challenging body regions such as web spaces of the feet or concomitant traumatic injury can make FB extraction difficult. Identifying the FB that requires referral and possibly operating room extraction is just as important as identifying which ones can be handled in the office.
CONCLUSION
Soft tissue POCUS is straight forward and management changing. POCUS identifies which patients require antibiotics, incision and drainage, and who can avoid unnecessary antibiotics and iatrogenic injury. Cellulitis creates a classic cobblestone appearance, where abscess has a typical anechoic appearance, and foreign bodies are hyperechoic with shadowing. POCUS will improve your practice and your patients will thank you for it.
REFERENCES
- Taira BR, Singer AJ, Thode HC Jr, Lee CC. National epidemiology of cutaneous abscesses: 1996 to 2005. Am J Emerg Med. 2009 Mar;27(3):289-92. doi: 10.1016/j.ajem.2008.02.027. PubMed PMID: 19328372.
- Hersh AL, Chambers HF, Maselli JH, Gonzales R. National trends in ambulatory visits and antibiotic prescribing for skin and soft-tissue infections. Arch Intern Med. 2008 Jul 28;168(14):1585-91. doi: 10.1001/archinte.168.14.1585. PubMed PMID: 18663172.
- Tayal VS, Hasan N, Norton HJ, Tomaszewski CA. The effect of soft-tissue ultrasound on the management of cellulitis in the emergency department. Acad Emerg Med. 2006 Apr;13(4): 384-8. Epub 2006 Mar 10. PubMed PMID: 16531602.
- Dawson M, Mallin M. (2013). Introduction to Bedside Ultrasound: Volume 2. [iTunes Version]. Retrieved from https://itunes.apple.com/us/book/introduction-to-bedside-ultrasound/id647356692?mt=11
- Sarah Medeiros. Point of care ultrasound for soft tissue. The California DO. 2015

Nice narration … thank you
LikeLike