

Inexpensive, Reproducible Ultrasound Scrotum Simulators
INTRODUCTION
Acute scrotal pain can present in the acute care or primary care setting from multiple different etiologies including: testicular torsion, epididymitis-orchitis, trauma, infarction, hydroceles and hernias. Differentiating between these diagnoses based on physical exam alone is challenging and unreliable. Ultrasound is the diagnostic study of choice and in many cases can be performed at the bedside to facilitate diagnosis and definitive management.[i]
In all areas of medical education, inexpensive, reproducible, high quality tools for teaching clinical skills are in high demand. This is particularly true for learning a topic such as scrotal evaluation with point-of-care ultrasound (POCUS). POCUS for the acute scrotum is a relatively easy technique to learn, is high yield in diagnostic information, and can be fertility saving. However, learning and practicing the technique of scrotal ultrasound often requires standardized patients or learning initially on actual patients. Utilizing standardized patients is costly and restrictive on schedules. Learning initially on real patients is not ideal either. Presented here is a guide of how to make inexpensive scrotal models. The models were used to teach both medical students and emergency medicine residents.
TECHNIQUE
The major parts required to create these models are: large party balloons, long/thin balloons (often used to make balloon animals), water balloons, sugar-free Psyllium Husk (Metamucil), powdered flavorless gelatin, and a manual water balloon pump. You will also need a metal or wood skewer in order to create testicular rupture, garbanzo beans (or other bean) for masses, and cherry pits or another seed/nut for bullet foreign bodies. See appendix A for an ingredients list. Appendices B-G outline the detailed steps to create each scrotal model. A summary of the steps are as follows:
- Boil water as directed on the back of the gelatin box as if you were making Jell-O. This is often 4 packets of gelatin to 6 cups of water (Figure 1).
- Pour the hot water in a bowl and mix in the psyllium. The correct amount of added psyllium will make the water opaque where you cannot see through it, but not too much that it does not completely dissolve (Figure 2). This step is particularly important. Be mindful to mix the psyllium well until it is fully dissolved without clumps. [ii] [iii]
- Mix in the Gelatin as if you were making Jell-O. Mix until fully dissolved. This will make models that appear as normal testicles.
- For creating models that appear as testicular infarctions or ruptures (without actually rupturing them with the skewer) add half the amount of Gelatin as instructed on the box.
- For the appearance of masses or foreign bodies you may add beans, nuts, pits, etc to the water balloon before adding the psyllium/gelatin solution (Figure 3).
- Once the water cools some, without solidifying fill the water balloon pump with the solution (Figure 4). Fill the water balloons with the solution to desired testicular size and tie a knot (Figure 5).
- Next fill the same number of long/thin balloons with the same solution. Overfill a small portion of this balloon so it expands out. This portion can serve as the epididymal head. The long portion can appear as the epididymal tail, spermatic cord, or epididymal cyst if filled with water (Figure 6). Tie the balloon off.
- Tie the two balloons together, so they do not migrate too far from each other (Figure 7).
- Insert these two balloons together into the larger party balloon. This is best accomplished with two people.
- Fill the larger balloon with some water. This appears as a hydrocele on ultrasound, which adds pathology, but also aids in visualization of the testicle and epididymis (Figure 8). Tie the balloon off.
- For testicular rupture, do not add water, but instead rupture the water balloon with a skewer and tie the large balloon (Figure 9). Then insert into another large balloon and add water for a hematocele and tie off.
- Place balloons in the refrigerator overnight to solidify.
- In all steps be careful to remove all air.
DISCUSSION
The training session was preceded by a lecture on the acute scrotum and POCUS. During our training session we instructed learners on how to perform a standardized POCUS exam of the scrotum and contents (Figure 10). Several models were provided for learners and they took turns scanning and interpreting acquired images. Through the use of these models, trainees were able to gain comfort in evaluated the scrotum in a systematic fashion.
The models provided very good tissue mimicry. The models did require the use of ultrasound gel. Examples demonstrating the variety of models scanned with ultrasound are shown in figures 11-18. Although artificial in appearance, learners found it useful to have models for practice and pathology to identify. Novice learners seemed to differentiate normal appearing testicles from abnormal with relative ease.
One major limitation is that vascular flow could not be reproduced using these models. The technique, indications and common findings in testicular torsion and epididymitis-orchitis were discussed and demonstrated on the models (simulated). Cherries were used in these models to simulate masses and foreign bodies. They worked well to simulate metallic foreign bodies as they were more echogenic than expected. They functioned less well as masses and likely a material such as garbanzo beans (which do not have pits) may be better suited for this purpose.
It took approximately 3-4 hours of labor to make 12 models. The cost to make the models was approximately 20 US dollars. For the time and money spent, these models provided an excellent teaching experience for trainees and will be reproduced for future sessions.
CONCLUSION
POCUS for the acute scrotum is a relatively easy technique to learn, is high yield in diagnostic information, and can be fertility saving. One major barrier to utilizing the technique is lack of training opportunities. The models described here are inexpensive, easily made, reproducible, and provide examples of normal and abnormal scrotums. One major limitation is that vascular flow cannot be assessed.
[i] M Blaivas & L Brannam. Testicular Ultrasound. Emerg Med Clin North Am. 2004;22(3):723-48
[ii] R Bude & R Adler. An Easily Made, Low-Cost, Tissue-Like Ultrasound Phantom Material J Clin Ultrasound 1995; 23:271-273
[iii] P Khera & S Keshava. An indigenous model for learning ultrasound-guided interventions. Indian J Radiol Imaging. 2014; 24(2): 132–134.
Figure 1. Sugar-free psyllium husk and unflavored gelatin.
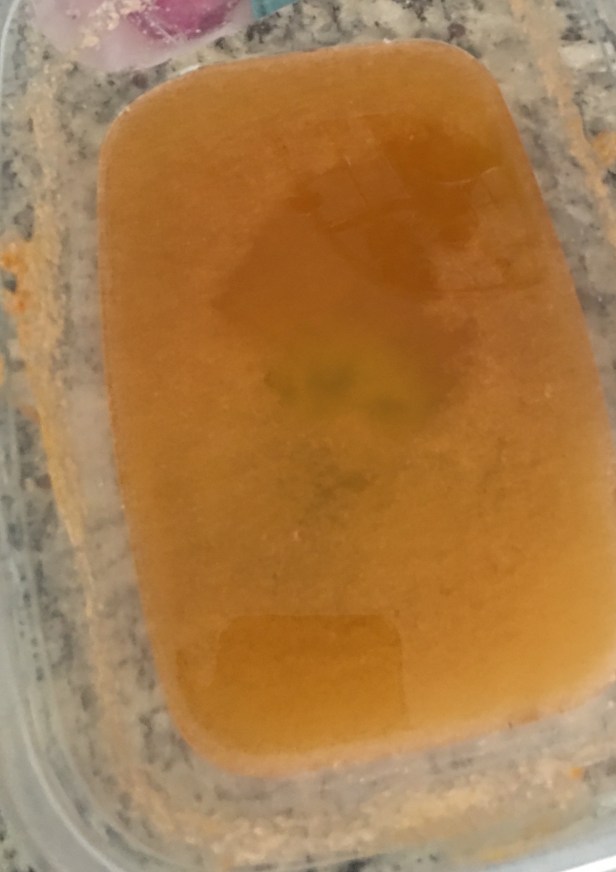
Figure 2. Sugar-free psyllium husk, unflavored gelatin and hot water not yet fully mixed.

Figure 3. Cherries placed inside the testicular water balloons to simulate masses and foreign bodies.

Figure 4. A manual water balloon pump used to fill the balloons sitting in the solution of psyllium, gelatin, and water.
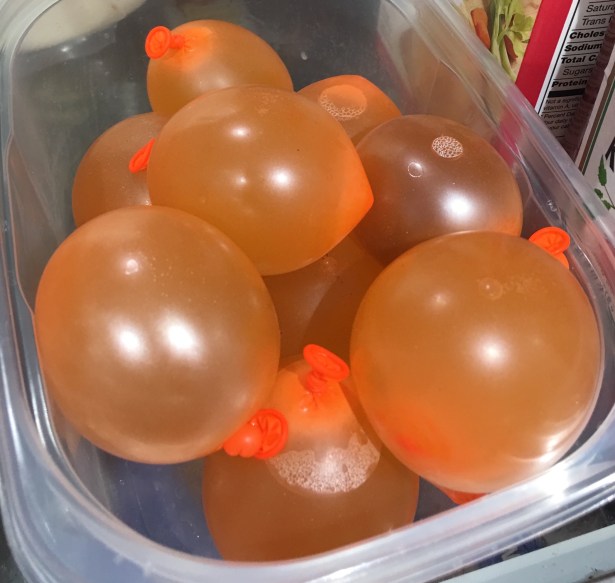
Figure 5. Testicular model: water balloons filled with water, psyllium and gelatin.

Figure 6. Long, thin balloons filled with the solution and projects from the model as the spermatic cord. Hyperinflated at one end for the epididymis. Five underinflated (orange) water balloons were used as masses and epididymal heads.

Figure 7. Long thin balloon and water balloon as epididymis and testicle respectively tied together before insertion into larger balloon.

Figure 8. Finished scrotal models.

Figure 9. A number of finished scrotal models with a skewer used to create testicular rupture models.

Figure 10. Trainees utilizing scrotum models during the training session.
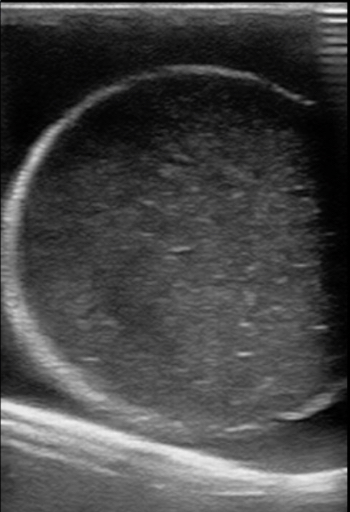
Figure 11. A model with normal testicle and a hydrocele.

Figure 12. A model with normal testicle, epididymis in view, and a hydrocele.
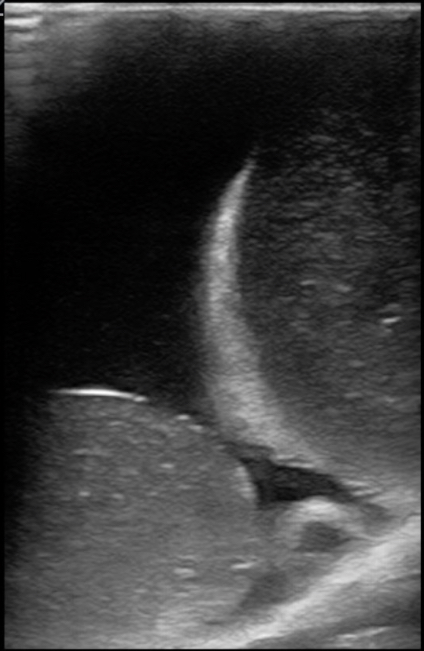
Figure 13. A model with normal testicle, large epididymis, and an epididymal cyst.
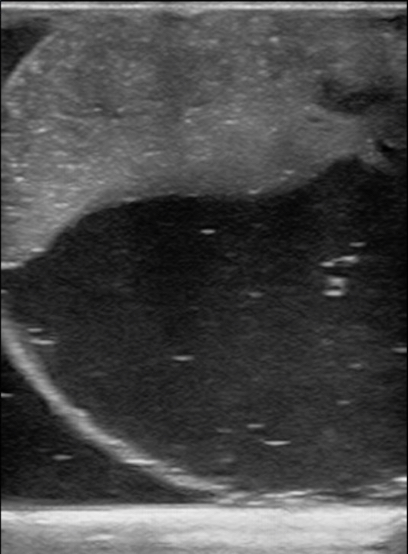
Figure 14. A model created with half the recommended gelatin concentration used as an example of testicular Infarction with hydrocele. The model was allowed to settle in place in the refrigerator and the psyllium collected to one side.
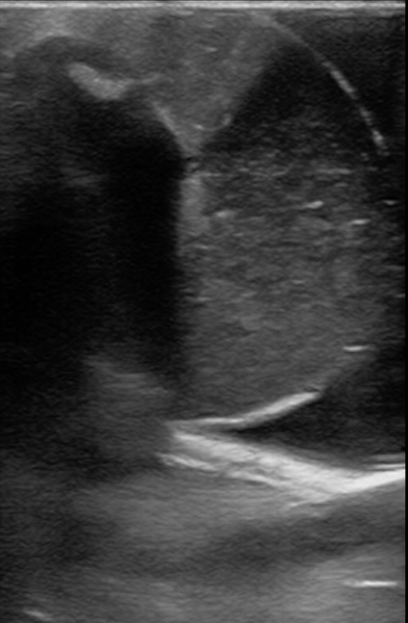
Figure 15. A model with a cherry and half the recommended concentration of gelatin used to demonstrate a penetrating foreign body with testicular rupture and hematocele.
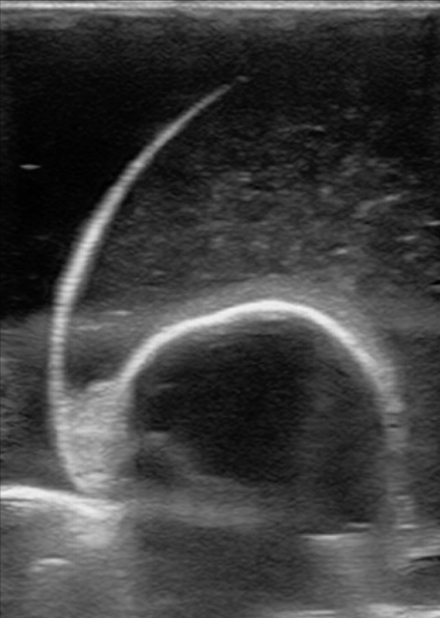
Figure 16. A model with a cherry placed with in the testicular model to simulate a mass or foreign body.
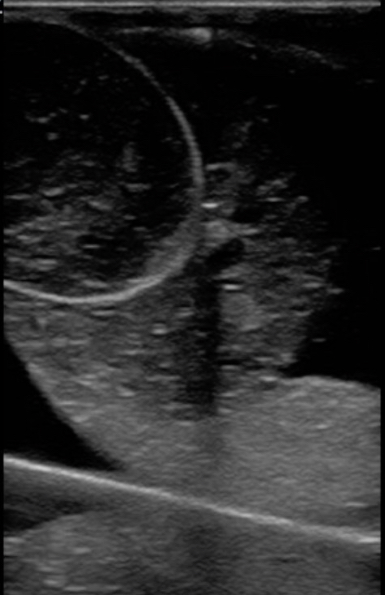
Figure 17. A model with an extra outer balloon and the inner contents ruptured with a skewer. Used as an example of testicular rupture.

Figure 18. A model with half the recommended concentration of gelatin used. Blunt trauma was then applied by bouncing the balloon gently several times and then placed in the refrigerator. The result was used as a model for testicular rupture, but did not require a skewer.
