
MSK POCUS
INTRODUCTION
Musculoskeletal (MSK) point-of-care-ultrasound (POCUS) is applicable in both the primary and acute care settings. It is more sensitive in diagnosing long bone fractures than plain radiograph. It aids in the assessment of tendons, diagnosing tendinopathy, tears, and rupture. It aids in evaluation of the muscle diagnosing tears, hematomas, and myositis ossificans. Finally, joints can be easily evaluated with ultrasound for effusion, dislocation, and associated fracture or soft tissue infection.
NORMAL ANATOMY
Figure 1 demonstrates normal appearing layers of soft tissue, fascia, muscle and bone. In general, the epidermis, fascia, and bone are hyperechoic compared to subcutaneous fat and muscle (which are hypoechoic). Bone will typically produce a clean shadow. Figure 2 demonstrates normal bony cortex in a long axis with shadow below. Muscle in a short axis is mostly hypoechoic with a few hyperechoic portions (Figure 3). In the long axis you can appreciate muscle fiber striations (Figure 4). Tendon in a long axis appears as a thin, well demarcated structure with striated fibers (Figure 5). Figure 6 demonstrates the principle of anisotropy, which is most apparent when imaging tendons and muscles. Muscle and tendon may appear focally hypoechoic depending on the angle of the transducer, but this is artefactual and will disappear with further interrogation. Figure 7 demonstrates a normal shoulder joint with no anechoic effusion and normal articulation of the glenoid and the humeral head.
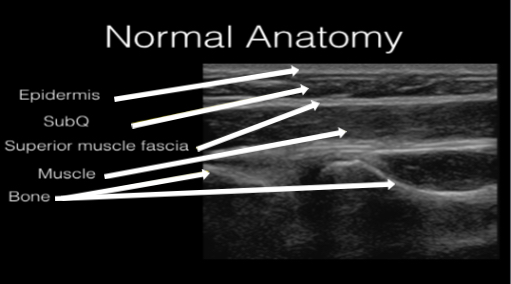
Figure 1. Normal soft tissue, muscle, fascia, and bone layers on gray scale ultrasound.
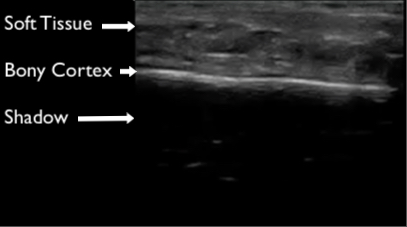
Figure 2. Normal long axis bone appearance on ultrasound. The cortex appears hyperechoic with shadow deep to the cortex.
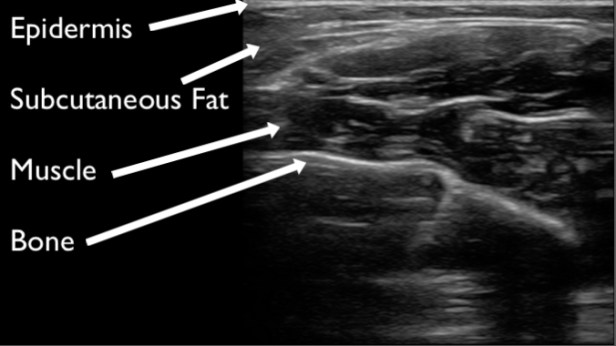 Figure 3. Demonstration of normal muscle on ultrasound in a short axis plane. It appears hypoechoic to fascia, epidermis, and bone. Within the muscle there are small hyperechoic portions that are layering of striated muscle, fascia, or neurovascular bundles.
Figure 3. Demonstration of normal muscle on ultrasound in a short axis plane. It appears hypoechoic to fascia, epidermis, and bone. Within the muscle there are small hyperechoic portions that are layering of striated muscle, fascia, or neurovascular bundles.

Figure 4. Demonstration of normal muscle appearance on ultrasound in the long axis plane. Its striated appearance demonstrating muscle fibers is pathognomonic.

Figure 5. Normal tendon shown with ultrasound in the long axis plane. Tendons appear as well demarcated striated structures that run from muscle and insert into bone.
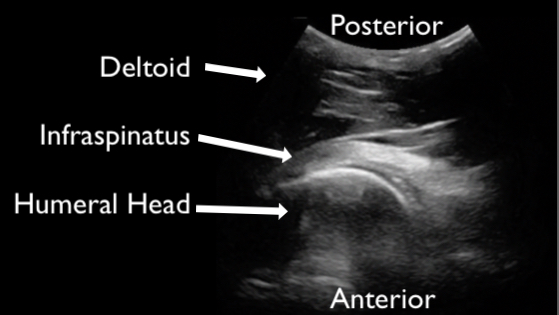
Figure 6. Normal tendon demonstrating anisotropy. Portions of the tendon appear hypo and hyperechoic because of the angle of the ultrasound beam. When further interrogated, these differences in echogenicity are no longer apparent.
Figure 7. An example of a normal joint. This still image of the shoulder demonstrated deltoid, humeral head articulating with glenoid, and the infraspinatus tendon. The image is acquired from the posterior shoulder.
GENERAL EVALUATION TECHNIQUE
During POCUS evaluation of MSK structures the clinician will uniformly use the high frequency or linear transducer. Use ample gel as often the conditions being evaluated are painful to palpation. All structures should be evaluated in two planes. All structures should be interrogated in their entirety and compared to the contralateral “normal” side of the patient. While evaluating the structure of interest, place two fingers from your hand holding the transducer to stabilize the probe on the patient. Optimize depth to 1-2 cm deep to the structure of interest and not further. Optimize the gain so that vessels appear anechoic. Using a dual screen mode may enhance your ability to perform side by side comparisons of structures (Figure 8).
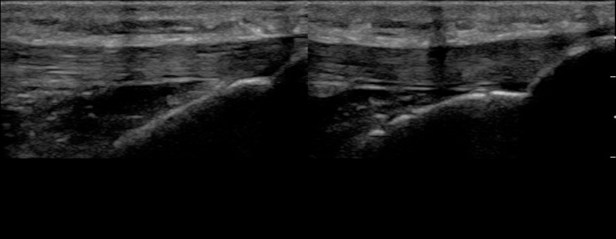 Figure 8. Demonstration of dual screen utilization. One Achilles tendon is imaged in the long axis and a still image is frozen. Then the contralateral Achilles tendon is imaged using the same technique. A side by side comparison can then be made and documented.
Figure 8. Demonstration of dual screen utilization. One Achilles tendon is imaged in the long axis and a still image is frozen. Then the contralateral Achilles tendon is imaged using the same technique. A side by side comparison can then be made and documented.
SPECIFIC EVALUATION TECHNIQUES AND PATHOLOGY
BONE
In general, fractures are easier to visualize while scanning along the long axis of the bone. Begin on normal bone and appreciate the bright white/hyperechoic bony cortex and shadowing deep to the cortex. Trace the hyperechoic cortex towards the region of pain and evaluate for disruption of the cortex. A break in the cortex is the fracture (Figures 9). Joint spaces may also demonstrate “breaks” in the cortex, but appear different than fractures with smooth borders and in predictable locations. When a fracture is identified take note of the angulation and displacement. You may freeze the image and measure the distance of displacement with calipers. Continue scanning to evaluate for other associated fractures or fragments. Remove the transducer and image the fracture from another surface to further evaluate for angulation and displacement. For example, if a fracture is identified while scanning a patient anterior radius also evaluate the fracture from the lateral aspect of the arm to appreciate how the fractured fragment is positioned in three dimensions. Lastly, hemarthrosis may be present and should raise the clinical suspicion for fracture even if one is not readily identified (Figure 10).
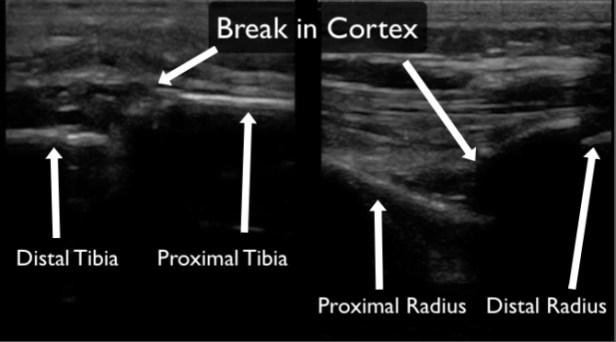
Figure 9. Examples of long bone fractures on ultrasound. Both imaged in the long axis of the long bone. The image on the left demonstrated a tibia fracture and the image on the right demonstrates a distal radius fracture. In both examples there are clear disruptions in the hyperechoic bony cortex.
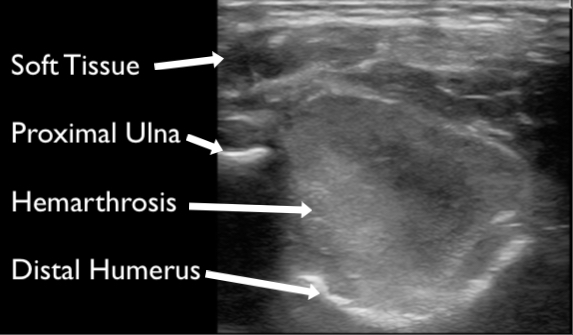
Figure 10. A large hemarthrosis visualized at the elbow in a grade one supracondylar fracture.
Tendon
Tendons should be interrogated in their entirety in the short and long axis to where they insert into the bone. The region adjacent to bony insertion is where the majority of pathology is identified. Complete or partial ruptures are readily apparent as disruption of normal striated tendon fibers often with associated surrounding hematoma (Figures 11, 12 & 13). Range of motion testing with simultaneous ultrasound can assist in evaluation for complete ruptures. Tendinopathy can be identified by the presence of calcifications (Figure 14), edema (Figure 15), and increased vascularity (when compared to the contralateral tendon). Edema will make the tendon more hypoechoic and larger in diameter compared to the contralateral tendon.
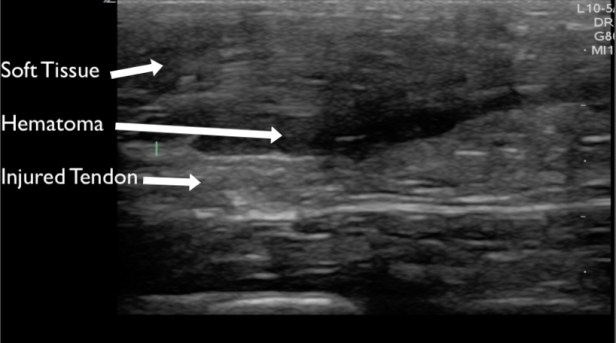
Figure 11. The Achilles tendon evaluated in the long axis demonstrating a partial or complete rupture with adjacent hematoma.

Figure 12. The patellar tendon evaluated in the long axis demonstrating a complete rupture seen at the proximal tibia with hematoma filling the space between the proximal tibia and patella.
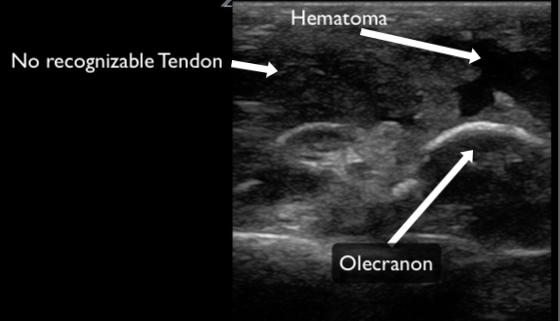
Figure 13. A triceps tendon evaluated in the long axis demonstrating a complete rupture. There is no discernable tendon and obvious hematoma present.

Figure 14. The Achilles tendon evaluated in the long axis demonstrating calcific tendonitis. Multiple small calcified portions in the distal tendon appear hyperechoic with shadowing.
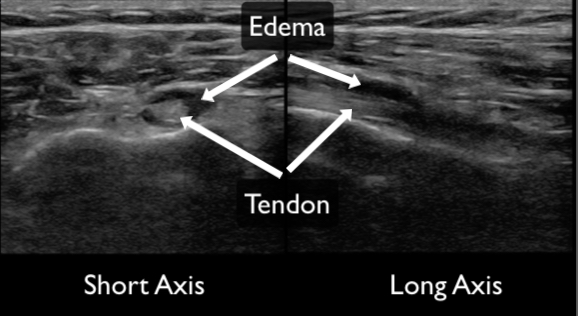
Figure 15. Tendinosis with surrounding edema demonstrated in both the short (left) and long axis (right). The edema appears as a hypo or anechoic ring around the tendon.
Joint
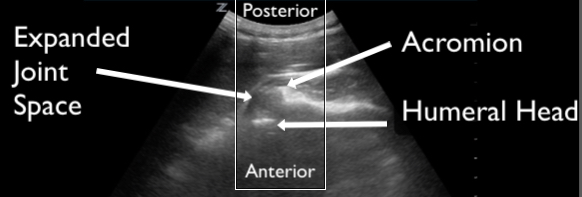
There are many joints that can be easily visualized with ultrasound and the technique varies based on the anatomical location and specific clinical question being addressed. Effusions appear as anechoic collections within and around joint spaces (Figure 17). POCUS is useful not only for identifying effusions, but for planning and performing joint injections or arthrocentesis. Tendon pathology is often identified near joint spaces at points of insertion. Finally, dislocation can be identified by appreciating abnormal articulation or gapping of the joint space (Figure 18). Evaluating the contralateral joint is helpful as a comparison of normal anatomy.
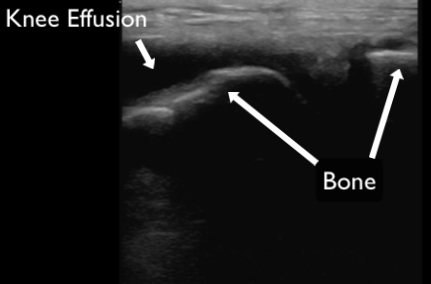
Figure 16. An anechoic collection of fluid identified as a joint effusion in a patient’s knee.

Figure 17. Demonstration of an anterior shoulder dislocation on ultrasound. The ultrasound transducer is placed on the posterior shoulder in the transverse body plane. The acromion and the humeral head are identified as labeled on the image. There is an abnormal space between the acromion and humeral head with translation of the shoulder away from the transducer, consistent with an anterior dislocation and hemarthrosis. Compare this image to the normal shoulder in Figure 7.
SUMMARY
Musculoskeletal POCUS has many uses in the primary and acute care settings. The exam is relatively easy to perform, does not have associated radiation, and can be performed serially to evaluate for clinical change. It is more sensitive than X-ray in identifying long bone fractures. POCUS provides sensitive and useful information when evaluating for muscle tears, hematomas, tendon ruptures, tendinopathies, joint effusions, and large joint dislocations. POCUS can further be used to guide joint injections and arthrocentesis. It is critical to evaluate structures in their entirety in two orthogonal planes and compare to the contralateral side.
